Intestinal Fibrosis in IBD: Rethinking the Inflammatory Paradigm and Emerging Therapeutic Opportunities.
Intestinal fibrosis causes strictures that can lead to obstruction and often require surgery; current drugs mainly reduce inflammation and do not reliably prevent or reverse fibrosis. Advances in understanding fibrosis mechanisms could point to new targeted treatments that matter for long-term outcomes.
Patients with Crohn’s disease or other IBD at risk for strictures, clinicians managing IBD, surgeons, and researchers studying fibrosis or drug development.
What To Know
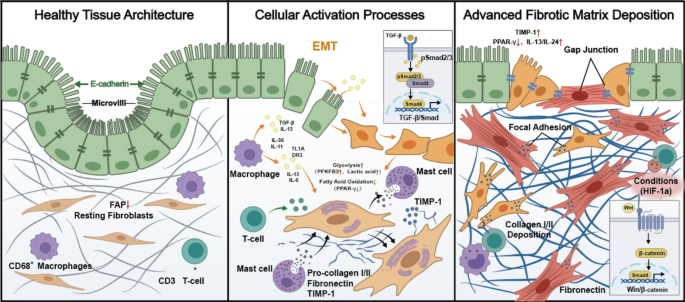
This review focuses on intestinal fibrosis in IBD — the process that leads to thickening of the intestinal wall and irreversible strictures, which often require surgery and worsen long-term outcomes.
The paper summarizes cellular and molecular mechanisms driving intestinal fibrosis, highlighting fibroblast activation, epithelial–mesenchymal transition, and interactions with the immune microenvironment as central processes.
It emphasizes that current medical treatments mainly target inflammation rather than fibrosis itself, and that surgery relieves obstruction but does not prevent fibrotic progression or recurrence.
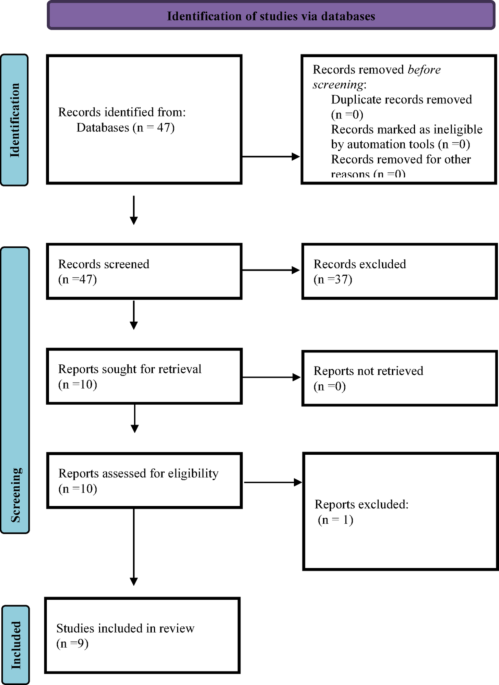
The authors outline that better mechanistic understanding could guide development of targeted anti-fibrotic therapies and help optimize clinical strategies; because this is a review, it synthesizes existing studies rather than presenting new trial results. This brief is grounded in the article abstract (structured content depth: abstract).
It summarizes the review’s scope and does not represent new clinical trial outcomes or treatment recommendations.
This source is a review article (abstract supplied) that synthesizes existing research rather than reporting new clinical trial results. Findings and therapeutic opportunities discussed are based on current evidence and remain subject to validation in clinical studies.