
Cureus
Cure8 research brief
Cure8 research brief
GI perforation is a serious, potentially life-threatening complication that can occur in people with autoimmune diseases; this report highlights that perforation can happen during corticosteroid tapering and that careful exclusion of other causes is important.
Patients with autoimmune disease on steroids; clinicians treating SLE or acute abdomen; surgeons.
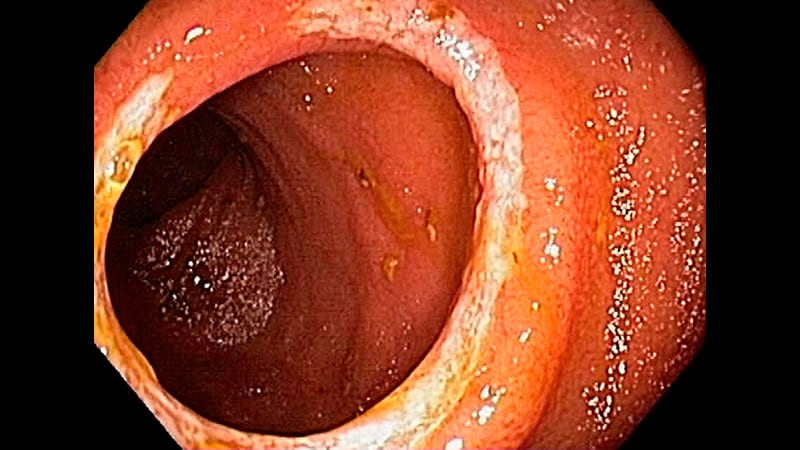
This case report describes a 62-year-old woman with systemic lupus erythematosus (SLE) who developed an acute mid-transverse colon perforation while tapering prednisone.
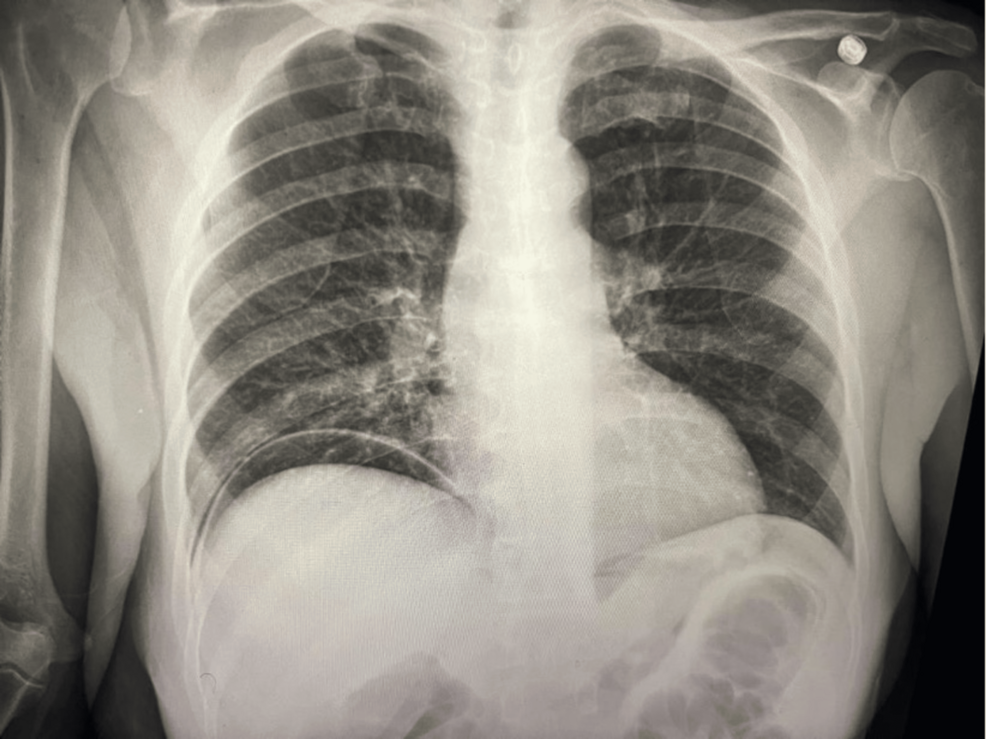
She presented with sudden severe right-sided abdominal pain, nausea, vomiting, leukocytosis, lactic acidosis, and pneumoperitoneum on CT; surgery revealed a solitary perforation treated with segmental colectomy and primary anastomosis.
Histology showed full-thickness ulceration with acute-on-chronic inflammation but no vasculitis, IBD, granulomas, or malignancy.
The authors treat corticosteroid-associated perforation as a diagnosis of exclusion and emphasize early source control (surgical management), thorough pathological review to exclude vasculitis or other causes, and postoperative reassessment of glucocorticoid exposure and steroid-sparing options.
The report is descriptive and based on a single patient; it does not establish causation between steroid tapering and perforation.
Single-patient case report summarized from the article abstract; does not prove causation between steroid tapering and perforation.
Review the original publication for the complete reporting, methods, and context.
This Cure8 brief is based on source text from the linked article. Cure8 is informational only and is not a substitute for professional medical advice, diagnosis, or treatment.
Reducing long-term corticosteroid use matters because steroids have significant side effects when used repeatedly or chronically. The study suggests ileocaecal resection may lower steroid exposure for many patients, but...
New treatment studies and biosimilars could affect future options and access to care. The piece also points out growing pediatric Crohn’s care and supports available (like an infusion center).
The article explains how gut bacteria may contribute to IBD and summarizes common tests and treatments people are likely to encounter. It highlights emerging microbial therapies (probiotics and FMT) that some patients...